





















I had the opportunity to synthesize my experience with and research on telemedicine into a Grand Rounds presentation at Highland Hospital in Oakland, California on March 11th, 2022.
The slide deck can be downloaded here.

Copyright Omar Metwally, MD.

I had the opportunity to synthesize my experience with and research on telemedicine into a Grand Rounds presentation at Highland Hospital in Oakland, California on March 11th, 2022.
The slide deck can be downloaded here.
Copyright Omar Metwally, MD.
Omar Metwally, MD University of California, San Francisco
If I were a government or private health insurance company trying to improve public health and reduce costs associated with treating cancers, chronic obstructive pulmonary disease, cardiovascular diseases, and many other preventable tobacco-related illnesses, how would I take on this challenge? Would offering nicotine addicts cash or subsidizing their insurance premiums curtail these unhealthy behaviors? While there’s some evidence that paying smokers works in the short-term, the effect is modest and has not been shown to be a successful long-term strategy. The 2017 recipient of the Nobel Prize in Economic Sciences, Professor Richard Thaler’s work demonstrates how humans’ bias toward short-term rewards contributes to poor long-term decision making. Especially in the case of chemical dependence, immediate positive reinforcement (e.g. a puff of a cigarette) trumps the relative abstractness of long-term planning. Who doesn’t want to live a long, healthy life free of suffering, expensive healthcare bills, and the loss of independence associated with frequent trips to the hospital? But to an addict, a drag from a cigarette is more attractive than the prospect of being rewarded with something like health, time, or disposable income in 10, 20, or 50 years time.
Breaking chemical dependence, and modifying behavior (such as a sedentary lifestyle, unhealthy eating habits, and compliance with preventive healthcare) in general, depends to a large extent on modifying one’s environment. This includes things like eliminating triggers (ashtrays, packs of cigarettes and lighters lying around), and enablers. More effective than paying someone to ditch unhealthy habits may be helping someone with an addiction change their social context. I’m skeptical about the efficacy of an incentive program that would, for example, pay smokers cash in exchange for urine tests that verify an individual’s nicotine-free status. The desire for long-term abstinence from substances, weight loss, or regular exercise must be intrinsic and reinforced by the company one keeps. A chronic smoker is more likely to smoke among a group of friends who also smoke than in an environment where they’re constantly subject to inconvenience, protest, or punishment whenever they reach for a cigarette. The corollary is the hypothesis that helping a smoker and their group of smoking friends quit together may be more effective than limiting an intervention to individuals.
Continuing the thought experiment, how does a health minister or surgeon general help people modify unhealthy behavior while changing one’s entire psychosocial situation? Instead of an intervention like a urine test, which people may find embarrassing or perhaps not worth the inconvenience of extra pocket money paid at the conclusion of a research study, what might a reward system look like which compensates individuals based on a convenient, dignified, and inexpensive “proof-of-motivation”? If I’m a smoker interested in quitting and make my intentions clear to my family, friends, and co-workers, could their vouching for me serve as such proof-of-motivation? If I truly muster the willpower to not smoke for a week, month, or year, could the people closest to me supplant something as sensitive/specific as a blood or urine test?
A hacker-mind will be quick to point out that a nicotine addict, if determined to do so, will find a way to game simple trust-based systems, whether it means stepping into -20C weather, walking for a mile to a secluded smoking spot, or sneaking cigarettes while driving to and from work. Moreover, a smoker could easily convince others to lie about their behavior in exchange for sharing the reward with colluders. What is necessary is a more perfect mechanism for allowing individuals to vouch for one another’s behavior. Earlier in my career, I had a tendency as a technologist in general and blockchain researcher in particular to reach for technology XYZ and ask, what can I do with this technology? I see this bias throughout Silicon Valley; we love to build things, and technology is an easy starting point for our desire to effect change.
The organizational and technological merits of my specialty’s distributed, peer-to-peer paradigms are rather clear. The other half of the blockchain equation, proof-of-work, makes sense in the context of value stores, a feature common to the two predominant cryptocurrencies (Ethereum and Bitcoin) — in addition to Ethereum’s Turing completeness and logic layer. In the excitement of embracing new technologies, one should be wary of shoehorning technologies into domains where a logical fit doesn’t exist. Bitcoin as a digital asset makes sense. Ethereum as a value store — and much of its organizational functionality — makes sense.
But with the goals of promoting healthy behaviors, helping developing countries kick a terribly addictive habit, and improving air quality as our starting point, how does one begin to effect change without burning up the planet’s resources in the process (one Bitcoin transaction wastes enough energy to power a household in a developing country for weeks)?
I would love the feedback of people thinking about this problem from different points of view. More than a billion human lives, which will be claimed by the tobacco industry in the 21st century, depend on it.

Omar Metwally, MD omar.metwally@gmail.com University of California, San Francisco DDASH - Ethereum Operating System for Knowledge Creation and Sharing ========================================== Github repository ----------------- Project website ----------------- First Draft
Abstract
This work bridges the technical concepts underlying distributed computing and blockchain technologies with their profound socioeconomic and sociopolitical implications, particularly on academic research and the healthcare industry. Several examples from academia, industry, and healthcare are explored throughout this paper. The limiting factor in contemporary life sciences research is often funding: for example, to purchase expensive laboratory equipment and materials, to hire skilled researchers and technicians, and to acquire and disseminate data through established academic channels. In the case of the U.S. healthcare system, hospitals generate massive amounts of data, only a small minority of which is utilized to inform current and future medical practice. Similarly, corporations too expend large amounts of money to collect, secure and transmit data from one centralized source to another. In all three scenarios, data moves under the traditional paradigm of centralization, in which data is hosted and curated by individuals and organizations and of benefit to only a small subset of people.
1. Introduction
In its current siloed state, data is a liability rather than an asset. The value of data depends on its quantity and quality. Organizations, including corporations, government, and academia, have few incentives to share data outside the context of selling it. For instance, advertisers use data procured from individuals’ browsing history and social media use (via internet service providers, social media and search engines) to create detailed profiles of individuals’ online behavior and spending habits and more effective sell products to unknowing consumers. While this paradigm fits naturally into a capitalistic society, these economics of data collection and transfer do not facilitate the generation or sharing of knowledge in the academic setting.
A typical university-based research group depends upon external funding to support its research activities. These funds often originate from governmental bodies, philanthropic organizations, or corporations and are difficult to secure [1]. Only a small minority of tenure track scientists ever becomes principal investigators, and a lab that is productive today can become defunct tomorrow if its principal investigator is unable to secure funding for laboratory equipment and supplies such as microscope parts, reagents, and to compensate technicians and trainees [2]. Principal investigators spend a majority of their time writing grant applications rather than participating directly in the process of knowledge generation [3].
It is often said that publications are the currency of academia. The maxim “publish or perish” applies to most research groups, whose work culminates in peer-reviewed publications with publication fees commonly amounting to several thousand dollars [4]. Moreover, these peer-reviewed publications are heavily biased toward so-called “positive results,” in which mathematical correlations between variables are described [5]. The vast majority of data produced by scientific researchers do not refute the null hypothesis; in a best case scenario, they are deemed “negative results,” and are discarded; in a worst case scenario, they are data that can’t be replicated, verified, or are outright fraudulent [6]. The result is the modern-day academic machinery. This severely flawed system, a victim of many conflicting economic forces, results in a tremendously inefficient workflow in which most grant money is wasted in the form of negative, and therefore unpublishable, results. Principal investigators spend a majority of their time trying to secure funding. The ultimate winner is the $10 billion business of academic publishing [6]. In this reality, data with the potential to produce vast knowledge is rendered into a vastly wasted opportunity to exponentially build on communities’ resources. Individuals’ roles are minimized by the centralization of resources in the hands of a privileged few.
2. Background
While the term “blockchain” has been touted to near-hysteria in popular media in the context of initial coin offerings and get-rich-quick schemes, an understanding of this data structure’s logic reveals the tremendous and fascinating socioeconomic implications of storing data on blockchain. In its most simplified form, a blockchain is a ledger [7]. The reason for blockchain’s natural association with financial derivatives lies in its ability to mathematically prove the authenticity of data and demonstrate proof of stake and proof of work [8].
The starting port for these use cases is the typical consumer, who is separate from (and often completely unaware of) the data collected about him or her. For instance, a customer’s online behavior is collected and used to up-sell the customer as much as algorithmically possible [9]. Customers have nothing to gain (and a few thousand dollars each year in extra spending to lose) from such data, which companies can sell to data brokers and merchants [10]. Analogously, the majority of taxpayers have no access to — and oftentimes no way to directly benefit from — publications funded through research that ends up property of academic journals [11, 12].
2.1 Case Study: Proof of Stake
Consider a research lab living from grant to grant, sifting through negative results to find crumbs of publishable positive results. If its lab notebooks were stored in the form of a blockchain, every experiment conducted, every machine learning model and dataset, and every clinical trial would generate data that lives on the blockchain as a cryptographic asset. Also referred to as “coins” and “tokens,” these cryptographic assets have inherent value because they are perfect receipts of the existence and transfer of data [13]. Never before in history has such a perfect ledger existed [14, 15]. On the blockchain, a relatively worthless set of negative results generated by a research lab becomes, when combined with negative results from thousands of other research groups, a trove of extremely valuable scientific data which can be traced to its owners whenever and however it is utilized. This large collection of negative results can become the source of unexpected positive results.
Moreover these blockchain-hosted data take on a new life as a financial derivative [16, 17]. These cryptographic assets, perfect receipts of the creation and movement of knowledge, can be traded by third-parties analogously to the way a company’s common stock is bought and sold on private and public marketplaces, albeit without the same regulations and on a different scale [13]. These tokens enable individuals, small and large groups alike to be compensated for their services in ways that are impractical or impossible in traditional economies [18]. Rather than relying on the slow and inefficient process of securing funding through grants, research labs can codify contracts on the blockchain to allow third-parties to bid for services and products rendered, on the metadata (what kind of knowledge research labs generate through their scholarly activities), and allow third-parties to become stakeholders in a research group’s success by directly benefitting from these research activities. For instance, if I believe that a particular group is contributing to science and society in a positive way, I can economically support this group by donating computing power and electrical energy to support the integrity of their lab notebook-turned-ledger, or by trading fiat for tokens representing proof of stake in their scholarly activities. What are today opportunities exclusive to accredited investors and institutions will become abundant opportunities for individuals to influence how perceived value circulates through society.
2.2 Case Study: Proof of Work
Consider the United States healthcare system, which still excludes millions of Americans from access to healthcare and financially ruins even more [19, 20]. Insurance companies are able to impose high premiums simply because they can. This is the logic of a capitalistic society, and insurance companies alone enjoy the benefits of owning valuable health data to their fullest extent — at the expense of those whose health data was collected [20, 21]. Imagine, on a smaller scale, a radiology group that puts a copy of every imaging study they do on a blockchain, along with a timestamp, a description of which type of study was done, and why it was performed. In doing so, data that would have otherwise been discarded can be engaged with by third-parties while directly benefiting the radiology group as well. For instance, grassroots-based health insurance co-ops could emerge from these sources of data which are otherwise privy to insurance companies, to the benefit of health consumers, who can undergo imaging studies and receive other healthcare services at a fraction of current costs. Information about which studies are performed — where, by whom, and why, and the result of those studies, can be used to lower healthcare costs while improving health outcomes, rather than raise healthcare costs and increasing profits.
One question that naturally arises, especially in the context of current centralized data paradigms, is: why would healthcare providers be incentivized to make public valuable data that is routinely used by corporations and insurance companies to maximize profits? One powerful force driving healthcare costs upward is the process through which health providers bill patients via insurance companies. Whether ordering relatively common drugs or expensive therapeutics or procedures, healthcare systems rely on administrators whose role is to submit authorization requests to insurance companies for approval to prescribe therapeutics on their patients’ behalf [22]. When a service is rendered in the hospital or in a clinic, a healthcare team is reimbursed a fraction of the amount they bill for, creating a cat and mouse game in which providers continuously bill as high as possible for services rendered with the expectation that they will only receive a fraction of what they bill for, and in which insurance companies place limitations on which drugs and services this will pay for and how much of the cost they will cover [23]. Blockchain would provide an end to this cat-and-mouse game and create a race to the bottom for healthcare costs, through price transparency and elimination of bloated administrative layers that handle authorization requests and billing, while creating a race to the top for healthcare outcomes as this ledger of health services and outcomes would be publicly accessible on a blockchain. Simultaneously, healthcare providers can immediately receive payment for services rendered, and although individual payments may be less, overall profits would increase because payments would arrive immediately and there would be no need for entire departments of administrators whose entire role is to maximally inflate bills sent to insurance companies (and patients, insured and uninsured) and to see these bills through collection.
2.3 Informing current and future medical practice
We may well already have all the knowledge we need to cure many illnesses currently considered incurable [24]. We may well have all the data we need to create intelligent machines that can interpret CT scans, diagnose disease, and synthesize drugs to cure any condition. The reason this knowledge hasn’t culminated in more rapid advancement in healthcare and science is that information is fragmented into pieces, siloed, and ultimately rendered worthless data. Blockchain allows transparent access to data. It would be naive to imply that a data structure will cure society of all its ailments. However blockchain allows data to culminate into extremely valuable information, once at the disposal of a powerful few, now to the benefit of all who become stakeholders by contributing to, interacting with, and propagating data.
3. The need for a ledger of scholarly assets
The need for this project, a protocol for the hosting and sharing of data on a distributed network (“Distributed Data Sharing Hyperledger,” or DDASH), arises from the observations by the above examples, as well as the observation that numerous research groups at UCSF and other academic institutions are working in parallel in their endeavors to create knowledge with little synergistic interaction [25]. How would research group A at UCSF Medical Center know that research group B at the University of Michigan is working to answer the same scientific questions, for instance? Without a transparent glimpse into which resources an organization owns and how they are being used and shared, both research groups miss opportunities for synergistic collaboration, within and among organizations.
Those acquainted with the politics of contemporary academia will be quick to raise several criticisms. Working within the current reality of Google, the most comprehensive collection of information known to humanity as of September 2017, why can’t research groups A and B simply host their digital assets — data and knowledge gleamed from this data — on websites or public databases? And if groups A and B are competing to be the first to publish in academic journals and competing to drink from the same pools of grant funding, why would any research group benefit by sharing the results of experiments that were costly to run before they can reap the benefits of publication and intellectual property [26]? The answer is in blockchain’s ability to capture proof of work and proof of stake in a network’s digital assets. There is nothing to stop a competing research group from stealing these data and benefiting at their competitors’ expense. Hosting data in the form of knowledge on a blockchain elegantly solves this problem through irrefutable mathematical proof of data ownership, transfer, and authenticity [27].
3.1 Distributed Data Sharing Hyperledger (DDASH)
DDASH (link to open source Github repository) is a ledger of scholarly data and knowledge produced by life science, informatics, and clinical researchers at UCSF and other academic institutions. The need for this project arises from the negative impact of data siloing, competition, and counterproductive financial incentives in the academic world on the creation and sharing of knowledge. Concretely, researchers can host data — datasets, experimental results, and machine learning models, among other examples of scholarly knowledge — on the distributed InterPlanetary Filesystem (IPFS) network and record the location of these assets on an Ethereum-based blockchain, along with a description of the asset, when it was created, and who has privileges to access the data.
3.2 Network Architecture
We believe that the IPFS protocol’s combination of security and speed is well suited for this application. IPFS uses content-based addressing, in which a hashing function determines a file’s network address based on the file’s contents [28]. Storing data in the form of a directed acyclic diagram (in this case, a Merkle DAG) results in trees that can be efficiently traversed and queried. IPFS is a peer-to-peer network in which data is continuously circulating through network participants’ machines which are running the client software. Data are rendered permanent by virtue of content-based addressing and persistent by virtue of its peer-to-peer architecture, and data are rapidly accessible without the bottlenecks that Internet Protocol imposes.
3.3 Blockchain as a ledger
The blockchain functions as a decentralized ledger of digital resources and the movement of these resources throughout the network. As the DDASH protocol is formalized, more robust mechanisms for associating IPFS hashes with the owner of the resource and the permissions granted by the owner are necessary. Currently the DDASH protocol accounts for the following elements:
In its current form, DDASH interfaces between the IPFS network and the Ethereum blockchain. One can conceive an alternative version of the DDASH protocol that seamlessly integrates a ledger-based indexing and permission management system, using for example IPFS’s native public and private keys and a native IPFS ledger. Keeping the networking architecture separate from the blockchain has tangible advantages, however, including the versatility of allowing users to create digital assets using any permutation of blockchains, private and public.
3.4 Security
DDASH allows users to manage access to privileged resources using public-key encryption. Public-key encryption allows users to identify themselves on the network using a verifiable public key, which can be used to encrypt resources such that they can only be unencrypted using a corresponding private key accessible exclusively to the intended recipient. Future versions of the DDASH protocol may feature ways to host resources on private clusters and manage access to these clusters on the blockchain. In doing so, resources are secured by limiting the movement of certain data to a subset of the swarm (network peers), and through a second layer of encryption. This not only allows data to move much more quickly through a network, it also greatly enhances security compared to the antiquated paradigm of data hosted on centralized, and therefore inherently vulnerable, servers. Common sources of wasted IT budgets and wasted productivity, such as forgotten, cracked and stolen passwords, or easily-intercepted HTTP network traffic, are obviated by virtue of the DDASH protocol. What stands between the theoretical underpinnings of this protocol and its implementation in academic centers and healthcare systems is not a question of the feasibility of this technology, but rather, whether legislation governing health information and computing will keep up with emerging trends in computing. Catastrophic beaches of sensitive consumer information, such as the Equifax data breach, have become regular occurrences and urgent reminders of the shortcomings of our antiquated Internet Protocol and undeserved trust in institutions that centralize large amounts of highly sensitive data at individuals’ expense [29].
3.5. DDASH Repository
DDASH is hosted as an open source repository at https://github.com/osmode/ddash.
We intend for this nascent project to illustrate the concepts and the larger vision outlined here while serving as a starting point for a formalized protocol for hosting and interacting with distributed digital assets. We made this a public repository early in the conception of this project in order to allow the codebase to benefit from the technical expertise and creativity of the open source community, and to allow the project to benefit from the rapid and exciting evolution in computing paradigms driven by the blockchain and distributing computing communities.
4. Using DDASH
DDASH currently runs on the blackswan private Ethereum network at 104.236.141.200. It benefits from the open source work produced by the IPFS, Ethereum, OpenPGP, web3.py, and py-ipfs communities.
The Go Ethereum client, web3.py, and py-ipfs Python packages are all prerequisite. The instructions here are for machines running Ubuntu 16.04. A Ethereum node must be connected to the blackswan private network and possess the ability to lock/unlock accounts to send transactions.
4.1 Directory Structure
Start by creating these directories:
mkdir /home/omarmetwally/blackswan mkdir /home/omarmetwally/blackswan/gnupg mkdir /home/omarmetwally/blackswan/data
4.2 Genesis Block
To connect to the blackswan network, you’ll need to use the same genesis block defined in genesis.json (see the Github repository). Move this file to /home/omarmetwally/blackswan/ and set your genesis block (you only need to do this once, and you need to install the Ethereum go client geth and Ethereum developer tools first):
geth --datadir=/home/omarmetwally/blackswan/data init /home/omarmetwally/blackswan/genesis.json bootnode --genkey=boot.key bootnode --nodekey=boot.key
4.3 Go Ethereum client and IPFS daemons
In order to use the web3.py and ipfs wrappers, you’ll need to run geth and ipfs daemons in the background, respectively:
geth --verbosity 1 --datadir /home/omarmetwally/blackswan/data --networkid 4828 --port 30303 --rpcapi="db,eth,net,web3,personal,web3" --rpc 104.236.141.200 --rpcport 8545 console
Be very careful when enabling RPC while your accounts are unlocked. This can lead to Ethereum wallet attacks, hence the recommendation to keep your development environment completely separate from any real Ether you might own.
The above command starts the go Ethereum client on your local machine and attempts to connect to the blackswan server at 104.236.141.200. Remember to set your genesis block according to the above directions. Trying to join this network with a different genesis block (such as the default genesis block) will not work.
Then open a new terminal window or tab and start the ifps daemon:
ipfs daemon
4.4 DDASH command line interface
Once your Ethereum and IPFS nodes are running, your account is unlocked, and you can interact with both clients, start the DDASH command line interface (CLI):
python main.py DDASH ::: Distributed Data Sharing Hyperledger ::: https://github.com/osmode/ddash Welcome to the DDASH Command Line Interface. [1] ddash> sanity check IPFS and geth appear to be running. [2] ddash> set directory /home/omarmetwally/blackswan/gnupg [3] ddash> new key [4] ddash> show keys [5] ddash> use key 0 [6] ddash> show accounts [7] ddash> use account 0 [8] ddash> set recipient your_recipient's_pubkey_id [9] ddash> set file /path/to/clinical/trial/data.csv [10] ddash> encrypt [11] ddash> upload [12] ddash> checkout QmUahy9JKE6Q5LSHArePowQ91fsXNR2yKafTYtC9xQqhwP The above commands: 1. check if IPFS daemon and Go Ethereum client are running 2. specify working directory (need to have read/write permission) 3. generate a new PGP keypair 4. list all PGP keypairs on your machine 5. uses the first (index 0) keypair as your identity 6. list Ethereum accounts 7. specify index of Ethereum account to use for transactions 8. specify an intended recipient's public key 9. upload the file to IPFS and create transaction containing the hash, user id of the person who uploaded the file, and recipient's public key id (or "public" indicating that it's not encrypted). 10. encrypt file from step 9 using public key from step 8 11. upload file from step 9 to IPFS network 12. check blockchain using IPFS hash as handle
4.5 Mining on the blackswan Ethereum network
Mining difficulty is currently relatively easy (1e6) on the blackswan network. Mine Ether by running:
geth --verbosity 4 --datadir /Users/omarmetwally/Desktop/blackswan/data --networkid 4828 --port 30303 --rpc 104.236.141.200--rpcport 8545 --mine console
5. Acknowledgements
I’m grateful to my mentor, Dr. David Avrin (UCSF) for his belief in this vision and for his unwavering support. My colleagues, Dr. Michael Wang and Dr. Steven Chan, provided formative feedback during the conception of these ideas. Steven Truong (UC Berkeley) inspired me with his technical creativity. Visionaries such as Vitalik Buterin and Juan Benet, and many brilliant minds contributing to the open source communities they inspired, conceived the technical underpinnings which are allowing these concepts to grow into powerful tools which I believe will transform and modernized academic research.
6. References
Since Ethereum’s conception, I’ve dreamed of a blockchain-based healthcare services economy and presented the idea at BitTorrent’s headquarters 3 years ago. It’s also taken me that long to conceive of a concrete study of this protocol’s readiness for the limelight. With Ethereum’s adoption by a number of blue chip companies, including JP Morgan and Microsoft, its inevitability is clear. While still unreachably abstract to many people, I believe that healthcare’s state of disarray is a perfect environment to test the waters. As I get ready to start a Clinical Informatics fellowship at UCSF Medical Center, I’m prototyping such a blockchain-based health services marketplace and would like to humbly present the proposal to the Ethereum community for its feedback.
Pricing for healthcare services is currently based on prices determined by insurance companies’ ability to negotiate price points with groups of healthcare providers, individual providers, and healthcare systems. The lack of a true free market, and insurance companies’ administrative overhead, contribute to inflated prices for healthcare services across the board. [Figure 1: Health services marketplace in the blockchain era]
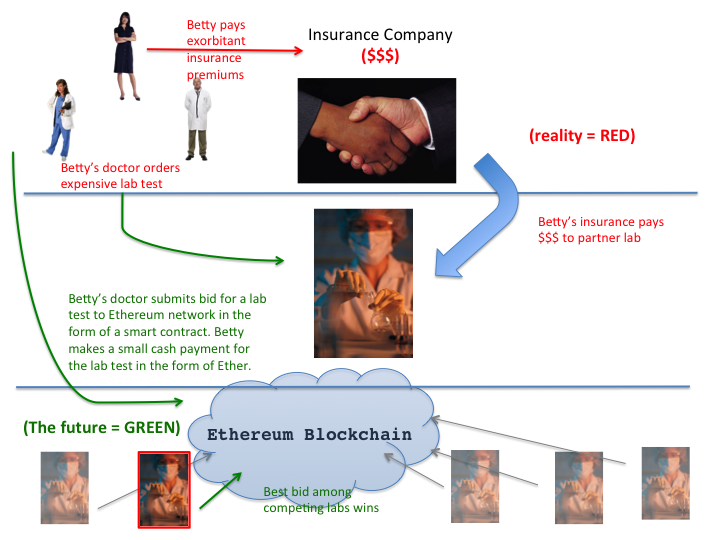
Figure 1: Health services marketplace in the blockchain era. Red text indicates how things work presently. Green indicates how things might work in a health services economy founded on the Ethereum blockchain. Notice the absence of insurance companies in the latter, hypothetical scenario. Their role has yet to be determined. I use laboratory testing as an example, but this would apply to imaging studies, office visits, surgical procedures, and consultations.
Enter Ethereum, a next-generation blockchain protocol for automatically executing “smart contracts.” Autonomously executed contracts obviate the need for escrow, attorneys, and administrators. Like Bitcoin’s protocol, Ethereum is a distributed blockchain that is open source, not owned by anyone, and runs off any and all computers running the client software. Ethereum’s novelty – and power – lies in the fact that it’s a Turing-complete system. Ethereum, unlike Bitcoin has mechanisms for executing logic, so smart contracts can be written by anyone, hosted on the Ethereum blockchain, and anyone in the world can interact with these contracts with the endpoint of manipulating data and moving money in the form of Ether (also a cryptocurrency).
So why not harness the Ethereum protocol to create a distributed, open source healthcare marketplace? Without administrative overhead (which accounts for the majority of an insurance company’s expenses, which are then passed on to patients and healthcare systems) and with the freedom for any provider of healthcare services to bid for a service (imaging, lab testing, consultations, procedures…), I hypothesize that the cost of healthcare services will be reduced to approximately 10% of its current artificially inflated price. Further contributing to cost and redundancy of healthcare expenditures is data siloing, the isolation of data on servers without APIs to set them free. Many healthcare providers will agree that it’s often much easier to repeat an expensive study than obtain records of that same procedure performed at an outside hospital (even if the study was just performed hours or days ago, and oftentimes, even if the study was performed at an affiliated hospital!). Ethereum’s distributed blockchain is a global ledger of everyone’s health information. I predict that sound security protocols, which need to be developed with healthcare’s unique needs in mind, will necessitate the use of biometric data to associate data on the blockchain with individuals.
So, how can we test the former hypothesis, that Ethereum can reduce the cost of healthcare services to 10% of their current prices?
I propose simulating such a bidding system to start collecting data on the free market prices Ethereum will foster by surveying physicians based in the community, as well as groups contracting with academic medical centers. If I survey Dr. Roentgen, Dr. Tomo, and Dr. Houndsfield (and a few hundred other radiologists) asking them if they would accept $X cash payment for imaging study A, B, or C (e.g. chest x-ray, mammogram, brain MRI…) performed STAT, tomorrow, or next month, we will start to approach theoretical market price for these studies.
If you are a fellow Ethereum developer or are otherwise interested in collaborating in the spirit of establishing healthcare as a human right on the Ethereum blockchain, please send me a line! I’m dreaming up experiments and am seeking partners in code.

[Daydreaming in Portland]
Omar Metwally, MD
Sunday April 30th, 2017
Portland, Oregon
Once Upon a Time a young man named Vitalik Buterin presented the concept of “Ethereum” to the cryptocurrency community. Vitalik became a Thiel Fellow and persuaded the world that there’s a better way to write laws, organize ourselves politically, and conduct transactions using a Turing-complete language built on the blockchain.
I would have never imagined, when I began developing on the Ethereum platform, that the concept of a decentralized autonomous organization (DAO) would make popular media headlines so soon. This is the start of something remarkable.
When I presented my vision for decentralized autonomous health insurance in June 2014 at the BitTorrent headquarters, Chris Peel, the founder of the Ethereum Bay Area Meetup, asked me how I would realize my vision. “Well…” I began, “operating health insurance is a big undertaking!” I said, scratching my head. Two years later, the time for a better way to insure our health and pay for health services is here. By cutting out the middle people, Ethereum-powered smart contracts and DAOs promise to dramatically reduce the cost of health services. Why should most of our outrageously over-priced health insurance premiums feed bloated corporations and their executives?
Ancient Chinese physicians practiced preventive medicine par excellence. In ancient China, physicians were compensated when their patients enjoyed good health, not when they grew ill – the opposite of our reactive, fee for service-based health system. Ethereum is our opportunity to end the healthcare crisis, and it’s incumbent on us to carry forth this effort.
DOCTOR WILL WORK FOR ETHER.
NOW ACCEPTING NEW PATIENTS.
Send me a line at omar.metwally@gmail.com
Omar Metwally MD
@osmode
20 minutes into her conversation with a patient with a diagnosis of irritable bowel syndrome (IBS), Dr. Zurcher realizes that she and her patient aren’t at all on the same page. With her own concept of “IBS” in mind, she tries her best to convey the fact that IBS is a syndrome characterized by constipation and/or diarrhea . Her patient, on the other hand, is less interested in discussing his constipation or medication for IBS than he is in bringing to his doctor’s attention his crippling social anxiety, which disrupts his life much worse than any of his gastrointestinal complaints. Dr. Zurcher’s grasp of IBS as a diagnosis established according to the Rome III criteria, while medically sound, has little to do with her patient’s conceptualization of his diseases, and unless she appreciates this, the encounter is unlikely to be productive.
As much as medical schools and residencies train physicians to listen carefully to their patients, physicians invariably approach the patient encounter with an agenda (to document a patient encounter, generate ICD-10 codes, and establish a problem list and plan) that doesn’t always coincide with a patient’s agenda.
To better understand how my patients conceptualize health and illness, I trained gensim’s word2vec implementation on 2 million disease-specific tweets. The beauty of this method is its capacity to uncover both obvious and less obvious semantic relationships among words. I challenge healthcare professionals to contrast their understanding of disease with their patients’ conceptualizations of illness.
Try searching for “heart failure”, “obesity”, “alcohol”, or “IBS”, for example. Each query returns the 10 semantically and/or lexically nearest neighbors in 100-dimensional space, along with their cosine similarity to the query term. The closer to 1.0, the closer they are in hyperspace.

The concept of cryptocurrency, and more broadly, of decentralized consensus, represents a shift away from the old-world paradigm of centralized authority. My parents’ generation (and their parents’ generation) grew up accustomed to confiding their trust in infallible governments, fail-safe banks, and reputable degree-granting academic institutions to which they paid decades’ worth of savings so that their children would have a better chance in society. Although decentralized consensus is silently changing the economic underpinnings of our society, I regard cryptocurrency and decentralized consensus as safeguards of the democratic ideals espoused by our constitution. The reality is that cryptocurrency is here to stay. Paradigm shifts are a constant in human history, and I believe that the emergence of decentralized consensus will mark one of the most momentous paradigm shifts in human history.
My friends and I went to hear Andreas Antonopolous, a cryptography and cryptocurrency guru, answer Bitcoin questions yesterday. If I were to summarize the 2-hour meetup in one sentence, it would be the following: the details of how cryptocurrencies are traded are still maturing, but the concept of decentralized consensus is here to stay. Decentralized consensus holds the promise of democracy 2.0, something that’s remained a Utopian dream except in the tiny country of Switzerland. Decentralized consensus holds the promise of a better world where governments and organizations don’t steal from politically weak, defenseless individuals. As Antonopolous points out, we’re fortunate enough to have a benevolent government in the United States, but the majority of the world is not so fortunate. Decentralized consensus holds the promise of empowering people to exercise the power of their vote to truly make healthcare a human right. Before I expound on this latter point, I want to outline some technical underpinnings for the uninitiated, so bear with me.
Satoshi Nakamoto’s most remarkable achievement with Bitcoin is the cryptocurrency’s success in solving the problem of a decentralized public ledger. In the case of the US Dollar or any other currency backed by a governmental body or bank, there exists a central authority that acts as the ledger. Bitcoin’s brilliance lies in the fact that the ledger is public, encompassing potentially everyone and anyone. The blockchain ledger is the communal ledger that lends cryptocurrencies their value. It’s characterized by the following 2 criteria [4]:
A Bitcoin comes into existence when a “miner” uses her/his machine (and therefore computing resources, disk space, and electrical energy) to generate new blocks that record cryptocurrency transactions. The block chain with the most cumulative computational work is accepted by consensus as the valid block. In other words, physical energy (electricity) is converted into Bitcoins. Keep that in mind if you ever find yourself wondering whether or not cryptocurrency is “a thing.” The reward for mining Bitcoins diminishes with time, as the horizontal asymptote of ~21 million BTC is approached (around 2024).
This setup has a few interesting results with regard to game theory. While mathematicians reading this will quickly pick up on the fact that wielding >50% of mining power holds the theoretical potential to manipulate the currency, game theorists should also note that this system strongly incentivizes cooperation and veracity [2] (I won’t get into the details here, but I’ll refer you to a suggested reading list at the end of the post).
The Bitcoin protocol is not Turing-complete. Enter Ethereum, a Turing-complete protocol for scripting contracts in the blockchain. Ethereum is big. If you’re not a believer yet in Vitalik Buterin and his work, I encourage you to check out the whitepaper for an interesting read. Ethereum uses a Python-like scripting language (Serpent) to convert contracts into cryptographic building blocks. For the first time in history, parties entering into agreements are not at the mercy of inherently biased third parties. Ethereum marks an era in which algorithms — not banks, governments, or individuals — hold the power to validate and execute contracts.
One interesting result of this decentralization is the so-called Decentralized Autonomous Organization (DAO), in which each member is represented as a cryptographic public key [1]. A contract that exists as lines of code in a Turing-complete language means that we can go beyond simple two-party agreements, like this prenuptial agreement written in Ethereum, to a corporate-like structure that automates redistribution of internal capital among participants in exchange for services provided, assets, or computational power. Transactions can contain information like votes, changes in the contract (such as amendments), or adding/removing members [1]. Most importantly, this is all automated without reliance on an escrow or central authority.
The U.S. healthcare crisis has demonstrated how lawmakers, insurance companies, and healthcare systems are struggling to figure out a way to fairly distribute access to healthcare. The U.S. healthcare system was hurt by an incentive system that rewards procedures rather than quality of care and health outcomes. Recent changes in CMS reimbursement are starting to change this, prompting the emergence of Accountable Care Organizations that receive payment in exchange for providing healthcare to a fixed population, rather than on a fee-for-service basis. The healthcare system failed for the same reason the financial industry lost its credibility in the 2008 financial crisis: third parties succeed in manipulating an easily manipulable system in their favor. People were robbed blind.
I’ll give a simple example of what I’ll call Decentralized Autonomous Health Insurance. Let’s say individuals A through J enter an agreement with physicians X and Y, in which X and Y agree to provide healthcare to individuals A-J. Let’s say in this simplified example that X and Y are not reimbursed for their services, but by A-J’s health outcomes (in ancient China, physicians were paid when their patients were healthy, not when they were sick). Let’s also say that X & Y have a practice that accepts cryptocurrency as payment. Then, A-J and X&Y can pen a virtual contract with the following stipulations:
We might even imagine a scenario in which each patient’s medical record is encoded and distributed in a decentralized manner such that it exists as undecipherable bytes among millions of computers around the world, rather than behind the walls of a single healthcare system. For example, a chip could keep track of our health habits and automatically append these data to our blockchain-based medical records. These data (such as smoking and exercise habits) could then be integrated into the communal contract, so that sedentary smokers have to pay more Bitcoins per year than active non-smokers in order to receive care from X & Y. In this model, individuals’ health (not access to healthcare!) is the internal capital. Everyone is both a payer and consumer of healthcare, and everyone has the power to vote on the bounds and conditions of care provided. This type of Ethereum-based Decentralized Autonomous Health Insurance would have no administrative overhead, no bureaucracy, and no board of directors to decide who is healthy enough to be insured.
I’m less interested in the exact economics of the hypothetical example above than in the broader concept of decentralized consensus and the self-fulfilling social contract. It’s time to decentralize health insurance the same way cryptocurrency is decentralizing currency.
Cryptocurrency and Ethereum are a new social and technological frontier, which haven’t really reached mainstream yet. These young protocols still have to pass several important tests (such as reliable security mechanisms) and prove their scalability before they become widely used, but I’m optimistic. The future will be one shaped by knowledge, and less so by historical inertia. Decentralized Autonomous Organizations hold the promise of just distribution of scarce resources, including the most vital one of all: access to healthcare.
References:
[First published on my Quora blog on May 7th 2014]
From Google Glass to Misfit Shine, wearables refer to any hardware that can be worn around, hardware with which we interact in ways beyond the traditional keyboard and mouse/touchpad. Wearables are our daily companions, collecting information about our bodies and environments, adapting their behavior to our movements. Most of them sync via Bluetooth (or BLE) to our mobile phones. A related but different category of devices under the larger umbrella of the Internet of Things are so-called “there-ables” (a nice term used by Naveen Salvadurai).
But the reality is that wearables are still in their infancy. The term still means little to people in non-tech industries.
I started writing software in 1997 when my parents bought Sony’s PlayStation developer kit for my 12th birthday, the so-called Net Yaroze. Everything was written in the C programming back then. There was no Stackoverflow and no Googling around for sample code. When I couldn’t figure something out, I had to flip through a stack of reference manuals that shipped with the device until I eventually figured things out.
Nowadays languages like Python and Ruby are all the rage. I give credit to the open source community to the modularity of these languages, allowing people to write and contribute to libraries and frameworks that make writing software far easier than it was in the days of C. Developers can now focus on building things and rapidly prototyping rather than figuring out how to accomplish relatively low-level tasks like rendering graphics.
A similar phenomenon is emerging in the hardware world. The open source hardware community is vibrantly blossoming. Hardware hackers are sharing schematics of their creations online, and tools like Arduino, Raspberry Pi, and BeagleBone are helping engineers and non-engineers alike prototype their ideas and build devices that are turning the “Internet of Things” from a buzzword into a reality. Even Google announced a new modular phone, challenging consumers to rethink the lay “blackbox” view of hardware.
Hardware prototyping has become remarkably analogous to software development, thanks to the rise of open source hardware communities and modular prototyping platforms. This is a tremendous driving force behind the explosion of wearables. You need a team of skilled electrical, industrial, and software engineers, a good amount of capital, and a factory to manufacture a new line of activity trackers. But even the most popular wearable devices nowadays are increasingly being born as Kickstarter-funded prototypes on breadboards. The big challenge isn’t conceiving or manufacturing these wearables; the big challenge is identifying a compelling use case, and a hungry market.
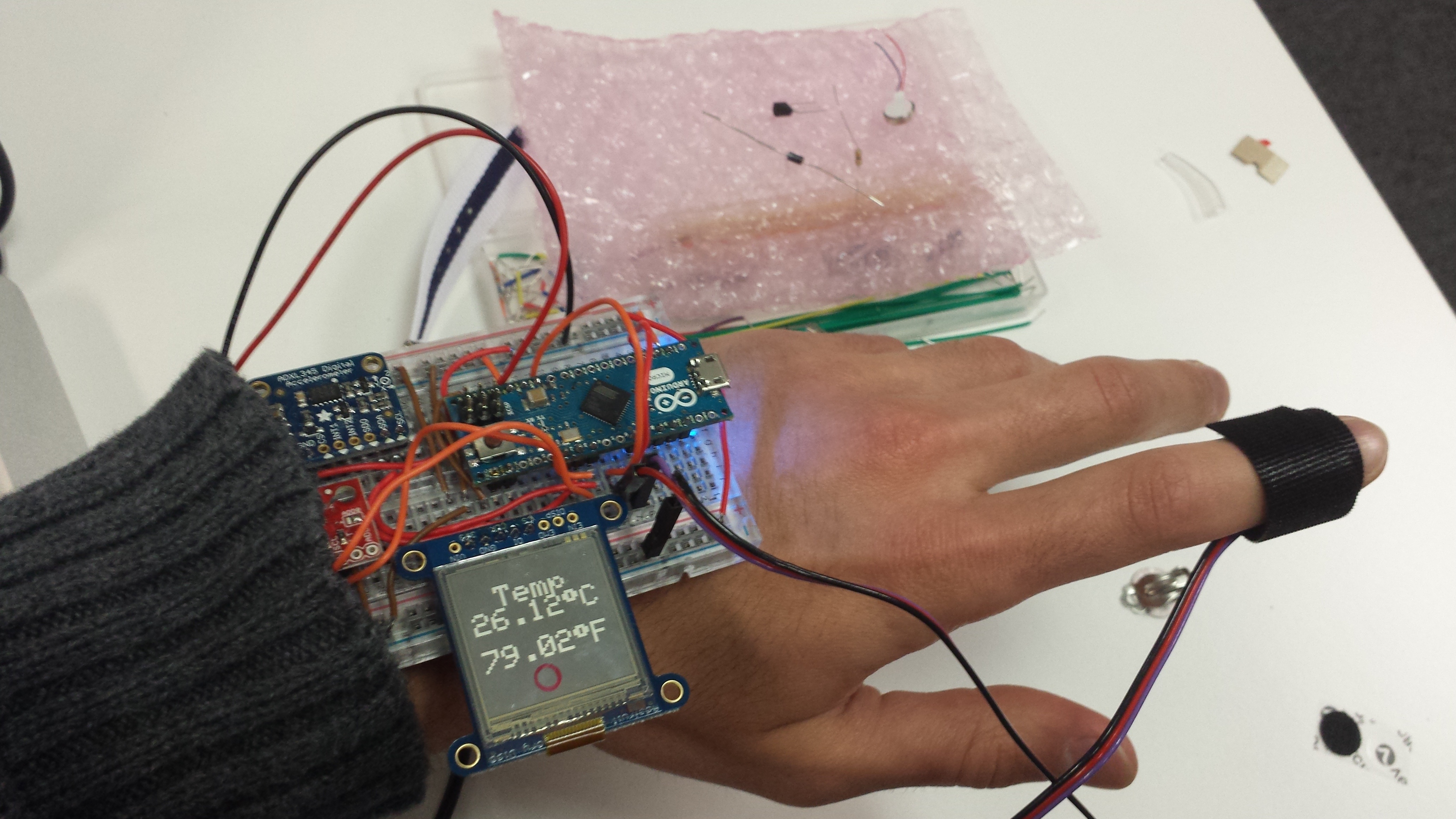
One group working heroically to make hardware accessible to all is iRoboticist. I spent the past weekend in an awesome 2-day workshop run by Saurabh Palan and his team expanding my knowledge about wearable hardware and getting inspired by smart, passionate hardware hackers from all walks of life. In a few hours, I built a smartwatch prototype that can display the wearer’s heart rate, temperature, and distance walked via a 3-axis accelerometer. Oh, and it also tells time.
The greatest act of rebellion is propagating knowledge. For the sake of knowledge.
Wearables are cool, but as iRoboticist founder Saurabh Palan points out, the greatest hardware of all is the human body, which continues to inspire engineers on a daily basis. No robot is as agile as a human. No app can recognize voices or images like the human mind. I’ve yet to see a robot that can repair itself when damaged.
I’ve come to believe that designers have the most important role in product development. My experience of co-founding PulseBeat and going through the Blueprint Health incubator have convinced me of this beyond a doubt. By designer, I mean someone who works to understand users and systematically studies how they interact with hardware and software. Someone who engineers not just graphical interface or the physical form of a device, but also its functionality. I hope that someday the position of a hospital’s Chief Informatics Officer won’t be filled by (semi-)retired physicians climbing the organizational ladder, but by true designers passionate about the interaction between patients, physicians, nurses, software, and hardware.
I’ll wrap up this post with a final thought on the most important of questions in tech entrepreneurship, the so-what question. From venture capitalists to physicians to journalists, people frequently ask me what I think about wearable technology and where it’s going. Technology is like the restless child running laps around our wizened, slow-moving society of bureaucrats and reactionary institutions. The majority of new technologies, regardless of how much Silicon Valley hypes them and infuses them with venture funds, never find a place in the real world. They either fizzle out or become sustenance for bigger fish. But that doesn’t matter — it’s part of the process of innovation. That’s why I chose tech over academia. Throw a lot of spaghetti against the wall until a strand sticks.
Building software and hardware is my passion. The Valley is filled with very talented engineers and hackers. It’s burgeoning with bullish investors eager to invest in new ideas and wide-eyed founders. But the most valuable thing I learned from my time at Blueprint Health was the fact that the biggest challenge any startup faces is not an engineering or funding question; it’s the so-what question.
We’ll eventually have miniature, implantable, and edible hardware with dozens of sensors onboard. But collecting data is not enough. Even doing analytics on these data is not enough. There’s a huge mismatch between sensors and actuators in health tech. It’s not enough to know that a patient’s health has changed for the worst. The trillion dollar question is, what will your app or hardware do to turn a patient’s health around, whether it’s delivering healthcare workers (what my startup does), delivering therapeutics, or changing people’s behavior.
So you built a cool app or a beautiful new wearable device. But what problem is it solving? Whose pain is it alleviating? To paraphrase Sam Altman, are you selling a painkiller or a vitamin?
We need to get patients, engineers, and healthcare professionals to sit down at the same table more often. The process of product development is radically different in health tech than in other industries. I think the reason so few people have really figured out health tech lies in the fact that it’s hard to get these 3 parties, who have disparate pain points, to participate equally in the development of consumer health apps and wearables. I’m working hard to change this.
[First published on my Quora blog on April 21st 2014]
Ask any healthcare professional to make one wish, and more often than not it’ll be something along the lines of, “I wish I had an app to write my notes for me.” Documenting patient encounters is time-consuming, annoying, and takes away time/attention that could be better spent communicating face-to-face with patients. This past weekend, I peeled myself away from PulseBeat-related work to spend the weekend in Boston participating in MIT’s healthcare hackathon. I went with Google Glass developer extraordinaire, John Rodley (TwiAge, a fellow Blueprint startup), and met several other talented people there. After 2 days of hacking, we walked away with a functional prototype of a Glass app that does just that — and won First Place. More importantly, I learned a lot and walked away feeling even hungrier to change healthcare as we knew it.
[First published on my Quora blog on March 18th 2014]

